Few clinical concerns frighten mental health providers more than the fear of being sued for malpractice related to working with suicidal patients.
In my professional life, I routinely train clinicians across the spectrum of mental health care. Over the past thirty years, I have trained thousand of mental health providers who practice in virtually all disciplines and treatment settings. As an Associate Director of Clinical Training in an APA-accredited clinical psychology training program, I have had countless opportunities to discuss the topic of suicide risk assessment and treatment with aspiring mental health providers. In all my years of teaching, training, supervising, and consulting, I have been struck by the concern that seemingly affects all types of mental health providers: the fear of malpractice liability pertaining to clinical work with suicidal patients.
Mental Health Providers Want to Know “How Do I Not Get Sued?”
Recently, I presented at a psychiatric grand rounds at a prestigious medical center. As often is the case with such engagements, I had a series of meetings with young mental health providers at this facility – psychologists, clinical social workers, and psychiatrists. In one meeting, I was introduced to a group of young providers, and they were invited to ask me “anything under the sun” about clinical work and suicide risk. After going around the room, the single most pressing question, by far, was, “How do I not get sued if a patient of mine takes their life?” We had an hour to talk about any topic related to clinical suicide prevention, and yet we spent fifty minutes talking about how to avoid getting sued.
This example underscores perhaps the most problematic aspect of the fear of malpractice liability related to treating suicidal patients. Namely, that mental health clinicians can easily become preoccupied with the perceived threat of malpractice and thus resort to defensive practices. In adopting a defensive posture, one may come to see the suicidal patient as a threat to one’s professional livelihood. Within this dynamic, the patient (and potentially the patient’s family) may seem like the enemy—an adversary who is ready and eager to sue if treatment goes south.
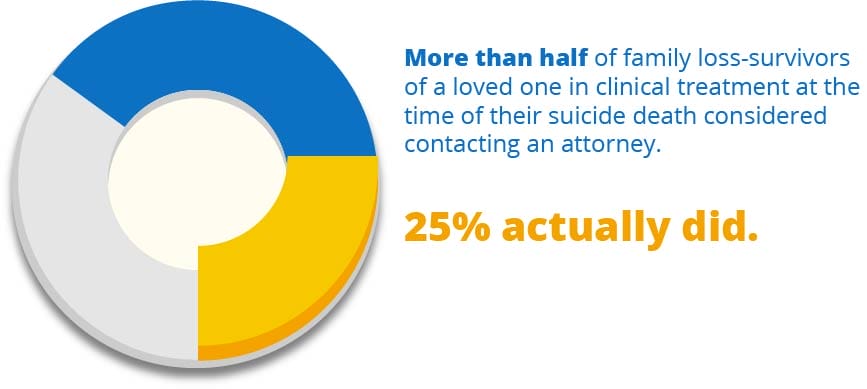
Fatal Suicide Outcomes Are Often Viewed as Malpractice
Early survey data has shown that when there’s a fatal suicide outcome of someone engaged in mental health care, the majority of family members studied considered the death of their loved one as an obvious case of malpractice. Indeed, within this survey, 25% of family members of people who had died by suicide contacted an attorney to pursue litigation for malpractice.
Reflecting on the topic of mental health provider malpractice, it is interesting to note that, within our culture, there is not the same routine presumption of negligent liability with other fatal outcomes following health care treatment. Certainly, with egregious examples, malpractice litigation is considered (e.g. a surgical procedure in which a surgical tool is left in the body). But despite the fact that we live in a highly litigious society, malpractice lawsuits are not routinely considered across health care delivery as they are in cases of suicide. There is one notable exception: Fatalities in childbirth that occur during delivery also often prompt the assumption of negligent malpractice. As a society, apparently, there is little tolerance for care that fails to prevent a self-inflicted death or the loss of an infant during childbirth. Even if the care provided was competent or heroic, a lawsuit might well be considered and pursued.
Fear of Malpractice Can Change the Way You Practice
In describing the topic of malpractice liability, I do so in full recognition that any death is a personal and family tragedy. But the concern that I am presently raising is how the fear of malpractice litigation can potentially paralyze an otherwise conscientious provider – leading to the proverbial deer in headlights. Such paralysis can lead to defensive practices in mental health care that might decrease the apparent exposure to malpractice risk but may have little to do with what is actually in the patient’s best interest.
As I have written about elsewhere, defensive practices within mental health can often lead to the overuse of inpatient psychiatric hospitalizations. Because of fear of malpractice, this type of “better safe than sorry” rationale often comes into play for patients who do not necessarily need this level of intensive intervention. In addition, there is often an overreliance – even a kind of wishful thinking – related to prescribing psychotropic medications to treat underlying psychiatric disorders of suicidal people. Despite the fact that the literature supporting the use of medicine to treat suicidality is limited or mixed at best, malpractice-related concerns may compel pursuing options that are extreme or ineffective.
If defensive practice is not the best way to avoid a malpractice suit, what is?
Definition of Malpractice in Mental Health Care
The answer to this question lies in understanding what constitutes malpractice. Briefly, malpractice is a tort action wherein a plaintiff (typically a surviving family member of someone who has died by suicide) engages a lawyer to argue that the defendant (the mental health provider) insufficiently met the “standard of care” and that what the provider did or did not do was a direct or proximate cause of the fatal outcome.
The standard of care for mental health providers is defined on a case-by-case basis by expert witnesses who attest to what a similarly trained clinician (with a similar case and in a similar setting) would do. An expert witness is hired by the plaintiff’s attorney to argue that the defendant did not meet this standard of care. The burden of proof lies with the plaintiff. In turn, the defendant’s lawyer hires their expert witness who argues that the mental health provider actually did meet the standard of care.
What ensues is an unpleasant process of discovery of records and relevant documentation, interrogatories, and depositions of the major parties within the case. Many, if not most, malpractice cases do not make it to trial—they get dropped or settled—yet the process of litigation can be traumatic for the defendant.
How to Decrease Your Potential Exposure to Suicide-related Malpractice Liability
More than twenty-five years ago, I published a journal article about how mental health providers can decrease their exposure to malpractice liability related to suicide. The glib answer was, and is, to save every suicidal patient! In reality, tragically, this is not always possible.
What one can do, however, is provide the best possible care, which is both suicide-specific and well-documented. This can be readily accomplish in your routine clinical practice by developing and adhering to “usual and customary practices” that focus on four key pillars of competent clinical care for suicidal patients.
These key pillars are:
1) Routinely and thoroughly assess for suicidal risk, and document that risk within the ongoing medical record.
2) If your patient is suicidal, there should be a sufficient focus on suicidality within the treatment plan, the use of a stabilization plan, and ongoing discussions about lethal-means safety.
3) As a competent mental health provider, you cannot “drop the ball” on the topic of suicide within the ongoing course of care. This means that the issue of suicide should be routinely assessed, treated, and well-documented.
4) You need to seek consultation on cases of potential suicide and document the consultative input.
Fatal suicide outcomes in mental health care are difficult for everyone involved, including families, providers, and organizations. But such outcomes are not necessarily legitimate grounds for malpractice litigation. There is no guarantee that by following these relatively simple steps, you will not be sued in the event of a fatal suicide outcome. But such routine practices can reduce one’s risk of malpractice exposure to negligible levels. This is because plaintiff attorneys take malpractices cases on contingency, which means they do not make a great deal of money unless they win or settle the case.
Skip Simpson, one of the nation’s leading plaintiff attorneys, has noted that if mental health providers follow the steps listed above and diligently document their practices, there is little incentive for malpractice lawyers to pursue litigation. Why? Because if a provider does follow these steps, the central litigation question becomes: Where was the negligence? Mental health providers are not expected to be mind readers or miracle workers, with unlimited control over the behaviors of their patients. But they are expected to be competent and to meet or exceed the standard of care.
CAMS Integrates “Competent Care” into All Clinical Care
While mental health providers can readily follow the recommended steps described above, the use of CAMS ensures that these basic steps of competent care are “baked” into their clinical care practices. CAMS, which stands for “Collaborative Assessment and Management of Suicidality,” is an evidence-based approach for the assessment and treatment of suicidal risk.
While I have seen cases in which patients who received CAMS-guided care have died by suicide, I have never seen or heard of a successful case of malpractice against a provider who adherently used CAMS. I have in fact seen on a few occasions that the use of CAMS has directly discouraged the pursuit of malpractice litigation. More to the point, I have directly seen or heard about countless cases in which CAMS successfully helped suicidal patients walk back from the brink of self-destruction.
Within CAMS-care, all of the members of our team are dedicated to reliably providing the best possible mental health care for patients at risk of suicide. In most cases, that will result in saving a life and averting the hardship that befalls families—and providers—who lose someone to suicide.