The recent end of the Spring 2023 semester marked my 40th year of working in the field of suicide prevention. During my first year in graduate school at American University, I took a remarkable class with Dr. Lanny Berman in the Spring of 1983. Lanny would soon become my major professor and the person who steered me into the world of suicidology. His course was entitled “Suicide, Death, and Life-Threatening Behavior,” and it was an eye-opening immersion into this important area of study. During that memorable semester, Lanny and I began a productive collaboration that led to my master’s thesis, my doctoral dissertation, many journal articles, book chapters, and a couple of books. Through my work with Lanny I had the good fortune to meet and work with many of the founders and heroes of the field, including Ed Shneidman, Bob Litman, Norman Farberow, Jerry Motto, and Marsha Linehan. Little did I know sitting in Lanny’s class all those years ago that my nascent interest in suicidology would evolve into a remarkably rewarding career that has been singularly dedicated to this important cause.
My Final Decade of Suicide Research
As I enter into my final decade of work in this field, I find myself at the ripe old age of 64 reflecting on the many challenges, abject failures, and dead ends that are inherent to the study of suicide. But through a lot of hard work, perseverance, and good fortune, there have been noteworthy successes. Chief among these has been the creation of CAMS and a rigorous line of clinical research to prove its effectiveness. And now with ten published open trials, seven published randomized controlled trials (RCTs), and two supportive meta-analyses, the question of whether CAMS works has been answered. The replicated and independent clinical trial data show that CAMS reliably reduces suicidal ideation (SI) and overall symptom distress, while it also consistently increases hope and decreases hopelessness. Of course, additional research questions still linger. For example, does CAMS reliably reduce suicide attempts and self-harm? And what exactly is the “secret sauce” of CAMS—the moderators, mediators, and mechanisms that make it work like it does? As for suicidal behaviors, I am delighted to note the publication of a new inpatient RCT of CAMS that was conducted in Germany showing that CAMS significantly reduced suicide attempts during the high-risk post-discharge period. Moderators, mediators, and mechanisms of CAMS are being further investigated within five ongoing RCTs of CAMS (and additional clinical trials of CAMS are now being developed). Building on this robust foundation of clinical evidence, our professional training company, CAMS-care, has trained thousands of clinicians across the nation and around the world. But from my perspective, perhaps the most exciting developments of all is the publication of the 3rd—and final—edition of the Guilford Press book, Managing Suicidal Risk: A Collaborative Approach. After two years of exhaustive work, this definitive source book on CAMS will prove to be a fitting capstone to the Guilford Press book series.
A Lack of Progress in Reducing Suicidal Suffering
While all these CAMS-related developments are exciting, I nevertheless find myself feeling frustrated and frankly impatient about the relative lack of progress overall within the larger field of suicidology. After 40 years of hammering away, I find myself craving more impactful changes and innovations to meaningfully reduce suicide-related suffering that can ultimately prevent this leading cause of death. So to this end, I would like to note and explore four particularly compelling big ideas that could make a meaningful impact as I further reflect on this field to which I have dedicated my professional life.
Focusing on Suicidal Ideation
Several years ago I found myself ruminating over the rejection of a manuscript from a peer review scientific journal. One particular reviewer pointedly dismissed various significant findings from a CAMS RCT because the intervention had failed to reduce suicide attempts. On the heels of this rejection, I began musing about the issue of “only” reducing suicidal ideation as a major criticism of CAMS. I then started to look at this critique differently. I began to question the behavioral bias that has dominated the field and I started to formulate an argument for the importance of suicidal ideation in and of itself. In fact, I have come to believe that reducing suicidal ideation may actually be a more important outcome vs. solely focusing on suicide attempt and self-harm behaviors. This train of thought was something that I had memorably discussed with my friend and colleague Dr. Thomas Joiner. I thus emailed Thomas and we ultimately wrote a well-received editorial entitled “Reflections on Suicidal Ideation” that was published in the journal Crisis—The Journal of Crisis Intervention and Suicide Prevention . In this piece, we argued that from a population perspective, that the biggest challenge we face in suicide prevention (by far) is the population of people who report “serious thoughts of suicide” in a given year. According to a recent SAMHSA (2022 ) survey, the population with serious SI included 15,600,000 American adults and adolescents in 2021 (the most recent year of data collection). Mind you, this number dwarfs the population that attempt suicide (1.7 adults in 2021) and is well over 300 times greater than the number of those who die by suicide. As Thomas thoughtfully noted, this is a profound level of human suffering. We argued that identifying and helping this enormous population upstream, could result in fewer attempts and suicides downstream. We consequently asserted that a shift in the field was needed to more fully appreciate and investigate the importance of SI as a means of decreasing this pervasive form of human suffering. Importantly, while there are excellent treatments that reduce suicidal behaviors (e.g., DBT, CT-SP, and BCBT) they do NOT reliably reduce suicidal ideation. Since this piece, we have endeavored to shift thinking within the field to meaningfully increase a focus on suicidal ideation within our collective research, clinical practices, prevention programming, and policy-related work.
Jaspr Health – Providing Hope during ED Visits
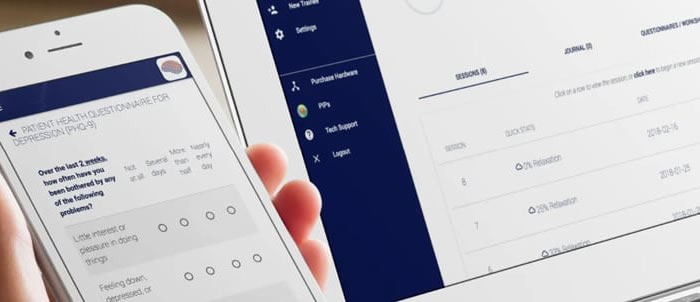
One summer day some years ago I was on a call with my colleagues Drs. Linda Dimeff and Kelly Koerner who were telling me about the successful use of an avatar named “Nurse Louis” and how this avatar-based technology demonstrated success related to discharge orders with medical surgical patients in a study conducted by Boston College investigators. The conversation evolved as we talked about the experiences of patients who are suicidal within emergency departments (ED) and I noted an extensive literature about how negative the ED experience can be for such people. This call became the genesis of a whole new avatar intervention that led to a NIMH-funded Small Business Innovation Research (SBIR) grant and the creation of an avatar based on my likeness named “Dr. Dave” that would be used to engage patients who were suicidal in the ED . Our novel tablet-based digital intervention integrated key elements of CAMS (among other related interventions from DBT and elsewhere). The striking initial success of this intervention was also in part due to the input of people with lived experience (of having been suicidal) which led to the integration of this important voice in developing the application and in the form of video testimonial stories of recovery and hope. Further NIMH SBIR funding led to an evolved intervention named “Jaspr Health” which was further shaped and refined based on input from a panel of people with lived experiences (and Dr. Dave was “retired” to my relief). Even though our RCT of Jaspr was cut short by EDs being overrun by Covid-19 patients, the obvious success within our underpowered clinical trial nevertheless provided ample and convincing evidence of the effectiveness of this novel intervention. Importantly, across my travels I have never heard of any ED experiences for patients who are suicidal being characterized as positive—not in the US, China, Uruguay, Australia, or throughout Europe. And yet with Jaspr, patients in the ED were having notably positive experiences and their Jaspr “favorites” could be downloaded to their smart phone for later use. Doctors get full reports based on CAMS aspects of the app which also ensures that certain Joint Commission institutional requirements are met as well. This remarkable line of innovation and clinical research is ongoing and reflects a fresh and exciting solution for a particularly infamous worldwide need—providing effective suicide-focused care in emergency departments for those patients who struggle with suicidal thoughts and behaviors.
The Hope Institute – Keeping Suicidal Patients out of the Hospital
Another undeniably compelling and recent development in suicide-focused clinical care is The Hope Institute that has been developed by my colleague Derek Lee in Perrysburg Ohio. The Hope Institute is an outpatient crisis setting that employs the use of both CAMS and DBT to stabilize patients who are suicidal using next day appointments (NDAs) and frequent visits (up to four times/week in some cases) to reliably stabilize patients in 5-7 weeks. The key within this model is that all care is suicide-focused and fundamentally evidence-based with proven clinical interventions. Perhaps most importantly, The Hope Institute singularly aspires to achieve stabilization as a worthy and valuable clinical goal in and of itself. Staff morale is high as clinicians do remarkable life-saving work. We are now in the process of standing up additional Hope Institutes in multiple different locations. The field needs this kind of model that emphasizes evidence-based, least-restrictive, cost-effective, suicide-focused clinical care to help people who struggle so that they can become stable and able to manage their suicidal thoughts, feelings, and behaviors. In my view, The Hope Institute is proving to be an exciting and notable clinical game-changer.
Mental Health Service Corp
Finally, I have been preoccupied with the idea of a “Mental Health Service Corp” since 2016. Given that 15.6M Americans wrestle with serious thoughts of suicide, we will frankly never have a sufficiently large and trained clinical workforce to begin to deal with the obvious and pressing needs of this considerable population (and research shows that many in this group do not want conventional mental health care). Given these considerations, a Mental Health Service Corp reflects one of my favorite pie in the sky big ideas that could significantly change the field. To have a Peace Corp-level national initiative to create a substantial paraprofessional workforce that could person the 988 Suicide & Crisis Lifeline, provide peer-support, work at respite and retreat centers for suicide stabilization, and with proper training and supervision even provide various evidence-based resources (e.g., safety planning, lethal means safety, and caring contacts) could have a profound impact. This concept was potentially under consideration by team members of the losing 2016 Presidential candidate. And while the concept did not play out then, it is nevertheless a compelling big idea that could be transformative if the political stars and will of the people were ever to align to make a significant difference in the larger suicide prevention workforce.
* * * * *
So, after 40 years, these are some of the big ideas to which I am drawn. I believe these ideas could make a meaningful difference for those who struggle in the most profound manner possible—considering suicide as an alternative to suffering. While progress is clearly being made, I am impatient. Far too many people continue to suffer, and too many people get hospitalized and medicated in ways that may not be helpful and might in fact be harmful. If we aspire to make a lifesaving difference, we must endeavor to think outside the box and fully embrace compelling big ideas to advance the field of suicide prevention.