It is interesting how ideas and constructs within suicide prevention that have been around for many years can rather suddenly become popular. For example, the notion of “lethal means safety” (LMS) has been around for as long as I have been in suicide prevention (which is now pushing 40 years).
We used to refer to LMS as “restricting access to lethal means,” but there was a sense that firearm owners might be sensitive to this language as a threat to their second amendment rights. And if there is one thing that is true in the world of suicide prevention, it is that words matter! The most striking example is “committing suicide,” which has now been banished within the field because of how it criminalizes the behavior (“die by suicide” is less stigmatizing). Indeed, recent LMS research has shown the referring to “firearms” is less off-putting to people who own them than the word “guns”—which is good to know! In any case, within contemporary legislation and policy, a particular emphasis on LMS has become red hot.
Understanding Lethal Means Safety
Simply stated, LMS broadly refers to any clinical, community-based, or policy-driven effort that literally blocks or hinders ready access to potentially lethal means that could be used in a suicide to end one’s life. The range of examples is extensive. In the United States, our #1 method choice is by firearm, and brilliant work has been done in recent years in this area by Mike Anestis at Rutgers, Kathy Barber and Matt Miller at Harvard, and Craig Bryan at Ohio State University. While it has been contentious, sincere efforts to engage the firearm community have led to some valuable shared perspectives that can be good for suicide prevention. But there are many other means, including hanging, jumping, drowning, helium “Exit Bags,” medications, razors/knives, carbon monoxide car exhaust, etc.
The Nuances of Lethal Means Interventions
Major population-level increases in suicides have been linked to certain lethal means. A decade ago, dramatic increases in female suicides in rural China were due to toxic pesticides. During the 1970s, Brits in the UK were using lethal coal gas fumes for suicides. These examples are well known because rather simple interventions that involved locking up pesticides and switching over to less toxic forms of coal directly reduced suicides in China and England, respectively.
Keith Hawton at Oxford did a clever study in the UK limiting daily access from pharmacies of over-the-counter pain-relievers and the use of blister packs that literally made it more difficult to gather a lethal dose (of the English equivalent to Tylenol) reduced overdose behaviors! My friend Konrad Michel in Switzerland has been the leader in the use of netting sites where people jump to their death.
During one family vacation, we visited a public park with Konrad at a palace in Bern where netting had been installed below a balcony of an infamous jumping location. Interestingly this net reduced suicide jumps to zero even though one can walk to the end of the balcony and jump off the side, but apparently, no one does this! So lethal means interventions do not have to be 100% foolproof; sometimes symbols of deterrence are quite effective.
Effective Lethal Means Safety Interventions
Within one early CAMS clinical trial, a patient lived in a group house where a loaded handgun was left on the dining room table for anyone that needed it! This was easily removed with the encouragement of the patient’s CAMS clinician. But then the patient had a prized knife collection and, when he became psychotic, he was tempted to stab himself in the eye (a rather gruesome method with uncertain lethality). He refused to surrender or give his beloved knives to another party for safekeeping.
Undeterred, the resourceful CAMS clinician bought him a metal box for his knives with a padlock and gave him the key. On top of his box was a taped copy of his CAMS Stabilization Plan. The patient was moved and grateful for this gift from his intrepid provider.
I once had a patient who almost jumped to her death but for a last-minute grab of her boyfriend (who I called to rescue her) as she started going over the railing. Following a two-week psychiatric hospitalization, we all agreed to have her life-saving boyfriend (who was a carpenter) build a wooden buttress to the sliding glass door to her balcony so she could not jump to her death.
Many of us who have seen suicidal patients over many years have countless stories of lethal means safety interventions that we have orchestrated that have made our patients immediately safer and less tempted by readily available lethal means. In my professional trainings, I often note that ready access to lethal means poses a “rival” approach to suicide-focused treatment for addressing the needs that underlie all potential suicides (e.g., unbearable suffering, isolation, financial ruin, etc.—what we call “drivers” within the CAMS Framework®). By removing temptation, the patient is more inclined to get needs met differently, more therapeutically, and the risk of suicide death decreased accordingly.
The CAMS Evidence-Based Approach to Lethal Means Safety
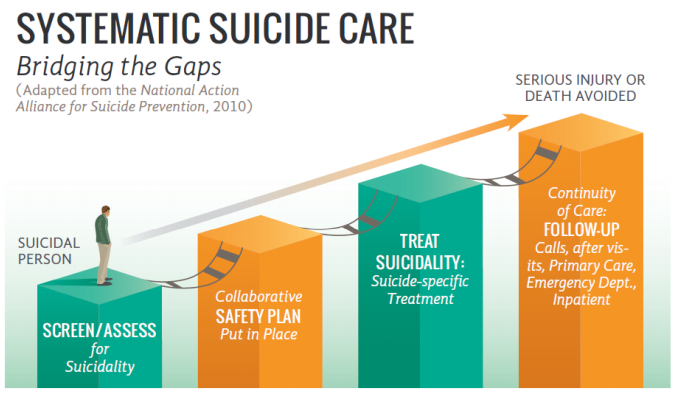
Within CAMS, lethal means safety is central to the evidence-based treatment framework. In fact, discussing access to lethal means is the first step in the CAMS Stabilization Plan. My friends Barbara Stanley and Greg Brown have developed the famous Safety Plan Intervention, which is a “first cousin” of the CAMS Stabilization Plan and Rudd and Bryan’s Crisis Response Plan. But in contrast to the CAMS Stabilization Plan, “Making the environment safe” is Step # 6 of the Safety Plan. The reason LMS is the first consideration of the CAMS Stabilization Plan is because of the differences between a one-shot Safety Plan Intervention and on-going treatment of suicidal risk, which is the emphasis in CAMS.
A common goal in “standard” CAMS is to keep a person who is suicidal out of the hospital if at all possible. In my view, the decision not to hospitalize a patient in CAMS is almost always rooted in the quality of the Stabilization Plan we are able to negotiate with the patient. If there is strong push back about lethal means, we may have no choice but to hospitalize. But if I can persuade a patient to surrender a stash of pills to their partner for safekeeping or convince another patient to use a cable lock on their firearm for the duration of our treatment, the need to hospitalize is often eliminated. We can then proceed in good faith to complete the balance of the CAMS Stabilization Plan, which focuses on different problem-solving techniques, who to contact in crisis, identifying people who will help decrease interpersonal isolation, and addressing potential barriers to receiving CAMS-guided care. CAMS Treatment® planning then concludes with a discussion of patient-defined drivers and how we plan to target and treat those problems and issues over the course of using CAMS. LMS is thus central to the CAMS Framework.
Unconventional Care Saves Lives
Several years ago, I was in the lab watching a digital recording of a CAMS session for fidelity purposes in our Army randomized controlled trial of CAMS. One of my favorite therapists in the study was working with a challenging case of a Soldier who had been repeatedly sexually assaulted. In turn, she kept a handgun in a side table drawer next to her bed for protection. However, her method for suicide would be to use this very firearm. She was emphatic that removing the gun was simply not negotiable because of the rapes she had endured—a definite therapeutic standoff!
The clinician thoughtfully considered the potential clinical standoff for a moment and then proposed the following: make a box to store the gun and to put a picture of the Soldier’s niece on the box as a reminder about why she should fight to live (her niece was her #1 Reason for Living on the SSF assessment). The Soldier readily agreed. I was worried, but the clinician felt confident in his intervention. In her next CAMS session, the patient brought in a work of art: a beautiful wooden box that she made in a shop with decoupaged images of the beloved niece! In my consultation with the provider, I pushed to swap-out the firearm with a taser, but the patient had zero interest in my helpful LMS suggestion! This remarkable woman responded beautifully to CAMS in 8 sessions.
In any final successful course of CAMS-guided care, there is a question about “what made the difference?” on the final outcome-disposition SSF. This Soldier, without hesitation, said, “CAMS showed me I could get my needs met without resorting to suicide…and you let me keep my gun!”