“I sure hope I can get her to come back so I can do CAMS with her. I think she would really benefit…but I’m afraid that she may have been scared off by our bio-psycho-social intake!”
This was said to me on a coaching call last week with a savvy Licensed Professional Counselor (LPC) I had previously trained, along with others who work with veterans and their dependents. This colleague was referring to the 19-year old dependent of a divorced veteran, who had been referred by her veteran father after she made a low-lethality overdose. The patient had just endured a 2-hour intake process required by agency policy, and this counselor was having trouble reaching her after her experience.
This account pains me greatly, and it is certainly not the first time I have encountered this problem – the effects of extremely long intake processes and administrative paperwork that most clinical settings require before any therapeutic care is provided to suicidal patients. I have been told by such agencies that “there are no exceptions.” So, even though a person is struggling with acute suicidal thoughts and/or behaviors, he or she must first endure hours of questions – some as inane as their birth order and whether they were delivered by forceps – before receiving any therapeutic assessment or suicide-specific treatment.
I believe there is often a unique moment, a window, of potential engagement that is squandered by unnecessarily long intake interviews and administrative paperwork. Administrative exceptions can and should be made for those who struggle with suicide. If we truly aim to clinically prevent suicides, the first touch experience for patients should be one of caring concern, empathy, validation, and truth – in other words, the CAMS assessment. I know this to be true because a published metanalysis proves that the CAMS assessment functions as a “therapeutic assessment” and further, we know from a randomized controlled trial (RCT) that suicidal patients prefer CAMS to usual care.
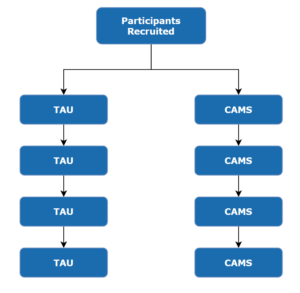
I face opposition to my position on the matter regularly. I win some, and I lose many. My first significant win occurred many years ago in a randomized controlled trial at a large VA Medical Center. In this instance, The Joint Commission’s “staff expert” was insisting on the first contact with the suicidal patient to be a 2-hour intake interview. The Chief of the service sided with me and agreed CAMS should be the first touch. I was thrilled to take the “win”.
However, at another large military medical center we were discussing how an abbreviated version of CAMS could be used in their emergency department, and the debate did not go my way. In this instance, not only was the provider arguing to initiate contact with a suicidal patient with an exhaustive intake procedure, but also stated “we could never engage on the topic of suicide so directly and quickly without forming a relationship first”, which he described as chatting about “the weather, sports, and the usual stuff”. I adamantly shared my opinion that such superficial chit-chat is ridiculous (it not only trivializes the seriousness of the patient’s suicidality, it is also transparently patronizing) and is no way to form a meaningful clinical relationship with a suicidal person.
As you might guess, I didn’t make many friends that day. Instead I was summarily dismissed, with the suggestion that I knew nothing about their military suicide patients and the challenges they faced. In truth, I have worked with suicidal military veterans for over 30 years, covering all four branches of the armed forces. I was appointed to a Veterans Blue-Ribbon panel by the Secretary of the VA, and to the Department of Defense Suicide Prevention Task Force. I was selected as a member of these investigative groups to become intimately knowledgeable of this “military suicide problem” in order to develop solutions. Finding the solutions was not the most difficult task – getting military mental health settings to implement them proved to be almost impossible.
The negative and vexing experiences these rigid and fruitless intake procedures cause simply must be reconciled with the reality of the challenges facing the suicidal person—and their provider—each time someone struggling seeks help that might avert a suicide outcome. The reality is that it is very scary for many to seek mental health care at all, let alone seeking care when one is contemplating ending their life by suicide. To be greeted by a stack of administrative documents and then subjected to an exhaustive “required” intake interview experience that may last up to two hours throws cold water on a patient’s motivation to seek care—it can be an instant turn off. Such requirements may close a window of opportunity to help save a person’s life through an evidence-based, suicide-focused treatment like CAMS. If we truly aim to clinically prevent suicides, the first touch experience for that patient should be one of caring concern, empathy, validation, and truth. Not data gathering and procedure-for-the-sake-of-procedure.
Our clinical experience and extensive research have shown that CAMS can be used to create a strong therapeutic relationship, forged in the crucible of the suicidal crisis. This is because CAMS providers go right into the patient’s suicidal struggle as they quickly engage with empathy, collaboration, and honesty using the Suicide Status Form.
I understand how people get comfortable with how things have always been done and fall into an “if it ain’t broke, don’t fix it” mentality. But what if it is broken? What if there is research evidence that proves it is broken, and by not fixing it many lives are lost? Shouldn’t we step out of this “comfort zone”? There are examples all around us of courageous people taking a stand to change policies that are wrong and harmful to individuals. It won’t be easy and it will be a long process, but those of us who believe in putting our patients first must fight for what the research is telling us and fix the currently broken mental health care system.
I will continue to beat this drum. In the meantime, for those mental health professionals who approach me with their challenges of how to effectively engage a suicidal patient when burdened with long intake interview requirements, I recommend that they not give up on the person. Follow up with the patient by phone or e-mail to get them to come back for a CAMS assessment and treatment. Additionally, when sending e-mail, include information about CAMS (Fact Sheet for CAMS Patients). Besides working to change the system from within, it may be the best we can do for now. Lack of purposeful and caring follow-up may result in lost opportunities, and I fear possibly lost lives.
I do hope that 19-year-old patient comes back to give CAMS a try – it could make all the difference in her world and give her a second chance at life.